IT IS, says Gabriel Demombynes, of the World Bank’s Nairobi office, “a tremendous success story that has only barely been recognised”. Michael Clemens of the Centre for Global Development calls it simply “the biggest, best story in development”. It is the huge decline in child mortality now gathering pace across Africa.
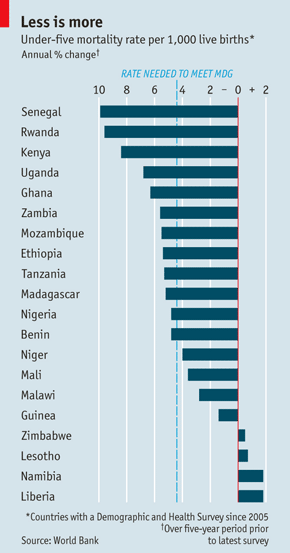
According to Mr Demombynes and Karina Trommlerova, also of the World Bank, 16 of the 20 African countries which have had detailed surveys of living conditions since 2005 reported falls in their child-mortality rates (this rate is the number of deaths of children under five per 1,000 live births). Twelve had falls of over 4.4% a year, which is the rate of decline that is needed to meet the millennium development goal (MDG) of cutting by two-thirds the child-mortality rate between 1990 and 2015 (see chart). Three countries—Senegal, Rwanda and Kenya—have seen falls of more than 8% a year, almost twice the MDG rate and enough to halve child mortality in about a decade. These three now have the same level of child mortality as India, one of the most successful economies in the world during the past decade.
The decline in African child mortality is speeding up. In most countries it’s now falling about twice as fast as during the early 2000s and 1990s. More striking, the average fall is faster than it was in China in the early 1980s, when child mortality was declining around 3% a year, admittedly from a lower base.
The only recent fall comparable to the largest of those in Africa occurred in Vietnam between 1985-90 and 1990-95, when child mortality fell by 37%—and even that was slower than in Senegal and Rwanda. Rwanda’s child-mortality rate more than halved between 2005-06 and 2010-11. Senegal cut its rate from 121 to 72 in five years (2005-10). It took India a quarter of century to make that reduction. The top rates of decline in African child mortality are the fastest seen in the world for at least 30 years.
The striking thing about the falls is how widespread they have been. They have happened in countries large and small, Muslim and Christian, and in every corner of the continent. The three biggest successes are in east, west and central Africa. The success stories come from Africa’s two most populous countries, Nigeria and Ethiopia, and from toddlers such as Benin (population: 9m).
You might expect that countries which reduced their birth rates the most would also have cut child mortality comparably. This is because such countries have moved furthest along the demographic transition from poor, high-fertility status to richer, low-fertility status. But it turns out that is only partly true. Senegal, Ethiopia and Ghana all reduced fertility and child mortality a lot. But Kenya and Uganda also did well on child deaths, though their fertility declines have stalled recently. So it cannot all be just about lower birth rates. Liberia, where fertility remains high, did badly on child mortality—but so did low-fertility places such as Namibia and Lesotho. The link between mortality and broader demographic change seems weak.
What makes a bigger difference, Mr Demombynes argues, is some combination of broad economic growth and specific public-health policies, notably the increase in the use of insecticide-treated bed nets (ITNs) which discourage mosquitoes, which cause malaria.
Ethiopia, Ghana, Rwanda and Uganda have been among Africa’s star economic performers recently, with annual GDP growth averaging over 6.5% in 2005-10. At the other end of the scale, Zimbabwe saw its GDP fall and mortality rise. This seems intuitively right. An increase in national income should reduce mortality not just because it is usually associated with lower poverty and better nutrition but also because growth can be a proxy for other good things: more sensible economic policies; more democratic, accountable governments; and a greater commitment to improving people’s living standards.
But growth offers no guarantees. High-mortality Liberia actually saw impressive GDP increases whereas Senegal, whose record in child mortality is second to none, had a rather anaemic growth rate by recent African standards (3.8% a year, half that of Rwanda). That what Mr Demombynes calls “the miracle of low mortality” has taken place in different circumstances suggests there can be no single cause. To look for other explanations, therefore, he studied Kenya in more detail.
And good riddance
Kenya is a test case. It has cut the rate of infant mortality (deaths of children under one year old) by more than any other country. It has had healthy economic growth (4.8% a year in 2005-10) and a functioning democracy, albeit after horrendous post-election violence in 2008. But Mr Demombynes noticed something else: it increased the use of treated bed nets from 8% of all households in 2003 to 60% in 2008. Using figures on the geographical variation of malaria, he calculated that half the overall drop in Kenya’s infant mortality can be explained by the huge rise in the use of ITNs in areas where malaria is endemic.
Bed nets are often taken as classic examples of the benefits of aid, since in the past they were pioneered by foreign charities. Consistent with the view that aid is vital, Jeffrey Sachs, an American economist, recently claimed that a big drop in child mortality in his Millennium Villages project (a group of African villages that his Earth Institute of Columbia University, New York, is helping) is the result of large increases in aid to villagers. In fact, argues Mr Demombynes, the mortality decline in these villages was no better than in the countries as a whole.
The broad moral of the story is different: aid does not seem to have been the decisive factor in cutting child mortality. No single thing was. But better policies, better government, new technology and other benefits are starting to bear fruit. “This will be startling news for anyone who still thinks Africa is mired in unending poverty and death,” says Mr Clemens. But “that Africa is slipping quickly away.”
Economist.com